
Electrocardiographic and Anatomic Analysis in Patients with Left Bundle Branch Block and Congestive Heart Failure
pp 425-436
DOI:
https://doi.org/10.7775/rac.v66i4.3415Keywords:
Bundle branch block, ECG, PathologyAbstract
Background Left bundle branch block is associated to a significant increase in mortality regardless of the severity of the underlying heartdisease. Material and method Forty one patients who died during hospital stay with clinical signs of heart failure New York Heart Association class III-IV were included in the study. Twenty six patients had persistent left bundle branch block (group I) and 15 patients had no evidence of ventricular conduction defects (group II). Sixteen clinical and anatomic variables were com-pared between both groups. In groupI patients QRS axis and other 12 electrocardiographic criteria were related to necropsy findings.ResultsCompared to group II, group I showed: 1) heavier hearts (562.8 ± 133 versus 446.4 ± 124g) (p< 0.01); 2) lower left ventricular shortening fraction (18.8 ± 3%versus 23± 7%) (p < 0.05); 3) higher prevalence of idiopathic dilated cardiomyopathy (34.6% versus 6.7%) (p<0.05); 4) higher prevalence of thickening of intramyocardial coronary arteries (88% versus 6.7%) (p < 0.00001). Patients with left bundle branch block and QRS axis? +120° were significantly younger than those with an axis<_-45°(47.2 ± 6.7versus85 ±15years)(p< 0.05). In regard to electrocardiographic analysis, only ST segment and T wave alterations showed good sensitivity (73%)and specificity (100%) for the diagnosis of acute myocardial infarction in the presence of left bundle branch block. The electrocardiogram showed low sensitivity for the diagnosis of left ventricular hypertrophy. Conclusions Our patients with left bundle branch block and congestive heart failure had: 1) diffuse ventricular damage without any particular cause to justify the QRS axis shift; 2) poor predictive power of the electrocardiographic criteria to detect an acute myocardial infarct or left ventricular hypertrophy, with the only exception of repolarization changes; 3) wall thickening of intramural coronary arteries with significant reduction of vascular lumen.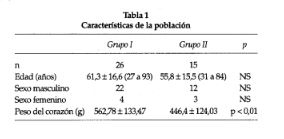
Downloads
Published
2026-03-12
Issue
Section
ORIGINAL ARTICLES
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









