
Percutaneous closure of left atrial appendage to prevent thromboembolism in atrial fibrillation
pp. 310-313
DOI:
https://doi.org/10.7775/rac.es.v80.i4.1493Keywords:
Left Atrial Appendage, Percutaneous Closure, Atrial FibrillationAbstract
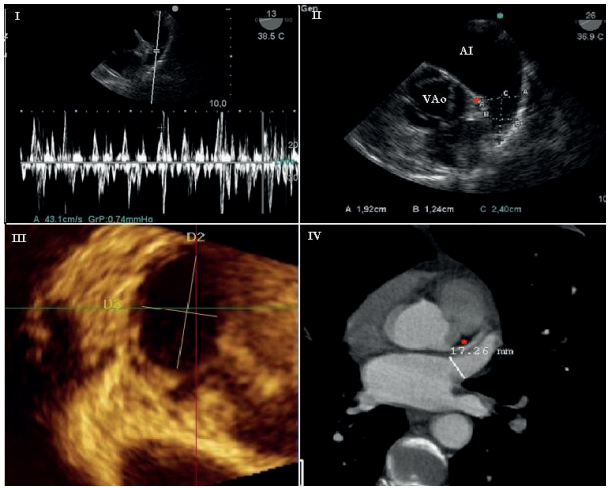
Background: Embolic stroke is a major concern in atrial fibrillation (AF), and anticoagulation is the therapy of choice to prevent it. Around 20% of patients with AF have contraindications for anticoagulation (OAC). The left atrial appendage (LAA) has been identified as the most common site of thrombosis in patients with AF, particularly in those with nonvalvular AF or impaired ventricular function. LAA occlusion reduces the incidence of embolic events in these patients. This article describes a case of percutaneous closure of the LAA with the Amplatzer Cardiac Plug device. The patient was at high risk of embolism and had absolute contraindication for OAC. The procedure was performed at the cardiac catheterization laboratory under general anesthesia with fluoroscopic guidance and transesophageal echocardiography, and complete closure of the LAA was achieved. During the procedure, no complications were reported. The patient remained event-free at three-month follow-up, with complete exclusion of the LAA. No embolic events have been reported.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








